Of all the amazing innovations taking place in healthcare, the use of robots in surgery is perhaps the closest to science fiction. For some it might conjure up images of the gleaming medical android that mended Luke Skywalker’s shattered face in The Empire Strikes Back; however, for many people, it’s an extremely disquieting concept. Submitting yourself to surgery is perhaps the ultimate loss of control and the thought of losing control to a machine, rather than a human, is a difficult step.
However, the object of robot surgery is in fact the exact opposite of surrendering to a machine, as the concept aims to restore control of the surgery to a human surgeon by playing to the strengths of both human and robot.
The demand for robot surgery has arisen from the increase of keyhole surgery - also known as laparoscopy; the technique of performing operations through two or three small incisions: one allowing access for a laparoscope - a combined light source and camera, or microscope, through which thesurgeon can see the operative site; and one or more for the surgical instruments.
This technique offers several advantages - namely that recovery times are faster as small wounds heal quicker than large ones; the need to slice through as much skin and muscle is removed, so rehabilitation is quicker; the chance of post-operative infection is reduced; and the whole process is, literally, less traumatic.
The students who pick up the skills best and fastest have one thing in common: they play a lot of computer games
However, for the surgeon, the advantages are balanced by a major disadvantage - keyhole surgery is very, very difficult. The surgical site isn’t open, so you can’t see what you’re doing, and you’re using tools and manipulators that, however advanced, are always less dextrous than the human hand. Because of the need to reduce trauma, incisions and stitches have to be very small, which is physically taxing.
The operations tend to take longer; if anything goes wrong it can be more difficult to correct and, for some operations, the risk of complications is higher.
And this is where robotic assistance is needed. Robots can, after all, accomplish some tasks more effectively than humans, especially where extreme precision or repetition is involved.
Robots don’t get tired, they don’t have hand tremors and they can follow instructions precisely.
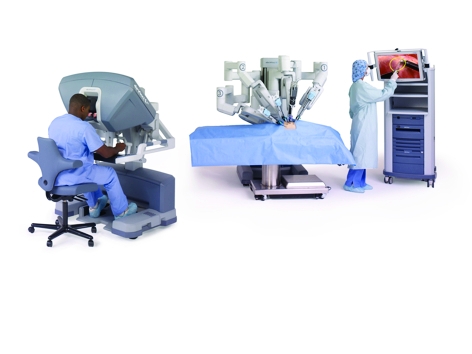
The best-known surgical robot is probably the da Vinci system, manufactured by Californian company Intuitive Surgical. Introduced in 1999, da Vinci is a telepresence device that is remotely operated by a human surgeon from a video-equipped workstation. The surgeon uses hand controls that operate four arms tipped with surgical tools.
Speaking at an event organised by the Institution of Mechanical Engineers, Prokar Dasgupta, professor of robotic surgery at King’s College London and a user of da Vinci, explained that the system has, in recent years, become widely used for prostate cancer surgery - especially when it is necessary to completely remove the prostate gland. Dasgupta, who practices at Guy’s Hospital, also said that da Vinci is extremely useful in preventing surgeon fatigue.
That sort of precise, repetitive movement is meat and drink to a robot
Patrick Finlay, MediMation
The system features tremor filtering, removing any shaking from the surgeon’s movements on the controls before transmitting them to the machine’s arms; and scaled movement, so that a movement of 1cm of the surgeon’s hands becomes a movement of 1mm of the robot’s manipulators.
This is important for suturing, for example. It means that the surgeon doesn’t have to make tiny, repeated movements to produce the very small stitches needed to rejoin the urethra to the bladder in radical prostatectomy,’ Dasgupta said.

However, da Vinci supplies no feedback to the surgeon and has to be operated by sight alone. ’This is a very

particular skill set and it takes a while to learn,’ Dasgupta said. It seems that the students who pick up the skills needed to operate da Vinci best and fastest have one thing in common: they play a lot of computer games. ’So we might have to say that if you don’t play computer games, you should probably go and do something else.’
In some cases, it’s useful to think of surgical robots not as replacement humans, but as machine tools. They perform a similar task - carrying out relatively simple tasks but with a precision unattainable for surgeons.
It’s in the area of orthopaedics that these types of ’robosurgeon’ are seeing the biggest developments. ’Orthopaedics are very well suited to using robots - simply because bones are hard and don’t move, so they create fewer problems than soft tissue,’ said Prof Klaus Radermacher of the University of Aachen, who is leading a team to develop a robotic milling machine for use in orthopaedic surgery.
Milling is an important part of surgery to replace joints such as hips and knees. Prosthetic joints are anchored in place with bone cement and all traces of this must be removed before the new joint is put into place. This can be done with hand-held tools, but it’s tiring work where the use of robots offers obvious advantages.
Orthopaedics are very well suited to using robots - simply because bones are hard and don’t move
Prof Klaus Radermacher, University of Aachen
Radermacher’s team is developing a modular milling system with interchangeable tool heads that is capable of milling away material in hip, knee or spinal surgery.
Reconfiguring the components changes the geometry of the tool so that it can work at the correct angles for each joint. Once the old prosthetic is removed, the tool first inserts an ultrasound probe into the bone cavity to determine where the remaining bone cement is. The surgeon then uses dedicated software to work out a tool path to grind away the cement and swaps the imaging head for a milling tool. The delicate, precise operation can then be carried out under human control, but without human intervention.
A similar class of surgery, ’needle driving’, refers to the insertion of any straight, rigid instrument into the body. This could be an orthopaedic operation, fixing pins, screws or drills to repair fractures.
However, it’s frequently used in soft tissues to perform a biopsy, drain fluid, implant drugs or other therapeutic agents at precise sites, or to locate electrodes to treat disorders of the brain, such as Parkinson’s disease. In all cases, it’s vital that the tip of the instrument gets to the right place within the body without damaging anything on the way.
These are widely used procedures, according to Patrick Finlay, managing director of robotic surgery developer Medimation, who claimed that, in 2006, more than 7.75 million needle-driving operations were carried out in the US alone.
Finlay explained that there are two types of needle-driving procedure - one where the needle can be inserted at any point to reach the target and one where the entry point and the target are fixed. For the former, the needle only needs to pan or tilt to reach the required trajectory, as well as moving in and out - three axes of movement. For the latter, it needs to tilt up and down, pan left and right, and translate along X and Y axes - five axes, including the in-out movement. But both of these modes are easily achieved by robots.
Robotic needle driving, like all robot-assisted, minimally invasive surgery, works in cooperation with imaging. The operation site is scanned using CT scanning or MRI and the exact target for the instrument tip is located by mapping the scan onto the patient. This stage, known as registration, is one of the most important parts of a robot-assisted operation.
The surgeon then indicates this point to the robot’s control system using a touch screen or stylus and the control system plots the best path for the instrument before adjusting its position. In many cases, the actual needle driving is done by the surgeon while the robot moves a guide tube into position and locks it in place.
The advantage of this, Finlay explained, is again the accuracy. ’If you’re doing a biopsy of a possible lung tumour and you’re inserting the instrument by hand, you can only reliably hit a tumour 1cm across. If it’s smaller than that, you can only advise the patient to come back in a few months and, of course, that isn’t desirable at all. But a robotic needle driver can reliably hit a spot 3mm across’.
Such a system could be particularly useful in one of the most challenging areas for any surgeon - operations on the brain. Advanced fMRI and CT scanning has given us unprecedented access to information about which areas of the brain are responsible for particular functions.
’For a surgeon trying to access a region of the brain, the problem is how to reach it with the same accuracy that he or she can see it, causing minimal collateral damage and taking as short a time as possible.’ It’s taxing, even for the coolest surgeon.
If you’re doing a biopsy by hand, you can only hit a target 1cm across. A robot can hit a spot 3mm across
Patrick Finlay, MediMation
One type of neurosurgery where robots could be especially useful is a form of cancer therapy where magnetic nanoparticles are inserted into the tumour in a 3D grid pattern, 3mm apart. After the entire tumour has been seeded, the area is subjected to a radio-frequency pulse that heats up the nanoparticles, killing the cancer cells.
’Imagine having to place all those nanoparticles by hand,’ Finlay said. ’It would take hours… but that sort of precise, repetitive movement is meat and drink to a robot.’
Despite these advances, robot surgery remains unpopular in the UK. According to Jonathan Gilbert, a colorectal surgeon at Wexham Park Hospital in Slough, patients tend to shy away from it. ’If I tell them that I’m going to use a robot, they assume that means that the robot will be doing the work and I’ll be on a golf course,’ he said. ’And I don’t even play golf.’
In fact, Gilbert uses a robotic surgical assistant that holds and guides his laparoscope according to his head movements. ’It returns control of the visual field to the surgeon,’ he said. ’It means that I don’t have to worry about an assistant pointing the camera in the wrong place and I don’t have to give instructions.’
It seems that we don’t have to worry too much about surrendering control to a machine in the operating theatre, which may evolve in a similar way to a factory - from a space crowded with people all using hand tools to a quieter place using dedicated machines. However, the point is to play to strengths. The machines will do what they do best, but humans will remain firmly in control.
Back story
Through the keyhole
The Robocast project aims to create a robotic system that will enable precision neurosurgeryThe EU project Robocast brings together several robot surgery projects to build a system for keyhole neurosurgery.
Bringing together lightweight robot arms - derived from research for orbital operation - with biomimetic flexible probes, the project aims to combine the remote operation possibilities of da Vinci with machine-tool-like precision and repetition.
Among those involved are the universities of Verona, Siena, Munich, Jerusalem and Karlsruhe, along with Imperial College, the Israel Institute of Technology and Israeli robotics company Mazor, which specialises in compact surgical robots that can be mounted directly onto the patient’s body.
Imperial College’s soft-tissue intervention and neurosurgical guide (STING) probe, which mimics the egg-laying organ of a wood-boring wasp, is part of this project and is designed to be steered through a complex path inside the brain, avoiding vital structures to reach the point of interest (read more about this here).
The Robocast partners also aim to develop systems for haptic feedback - something currently lacking in surgical robots.
This could be used to guide the surgeon away from vital organs by constraining movement, or to allow the surgeon to feel through a remote manipulator, as if they were operating by hand. This extra sensation would assist in suturing, for example, which relies strongly on a sense of touch.



Poll: Should the UK’s railways be renationalised?
All public service companies should be nationalised for many different reasons, particularly railways, not the least because the tax payer has already...